Writing a chapter for inclusion in Clinical Dermatology: From Diagnosis to Therapy
Although I had decided never to write another word about body-focused repetitive behaviors, I have to admit I was thrilled to be invited by Dr. Muhammad Jafferany to contribute a chapter to this book, which will be published by the APA in 2023. Why? Because I am so excited that the field of Psychodermatology will be getting more attention, and I can’t decline the opportunity to include my research into the efficacy of the psychodynamic approach into this book!
For those of you who aren’t familiar with the field, Psychodermatology is a combination of psychiatry and dermatology that has gained popularity in Europe over the past two decades and is gaining traction in the U.S. Some practitioners, like Dr. Jafferany, have degrees in both psychiatry and dermatology. The psychodermatology model is a team approach, in which a dermatologist, psychiatrist, and therapist all treat an individual struggling with body-focused behaviors such as skin-picking, hair-pulling and cheek-, nail- or lip-biting.
Dermatologists treating these disorders discovered that connection between mind, skin and emotions means that skin disorders contribute to difficulties with mental health and, conversely, mental health conditions can lead to negative interactions with the skin.
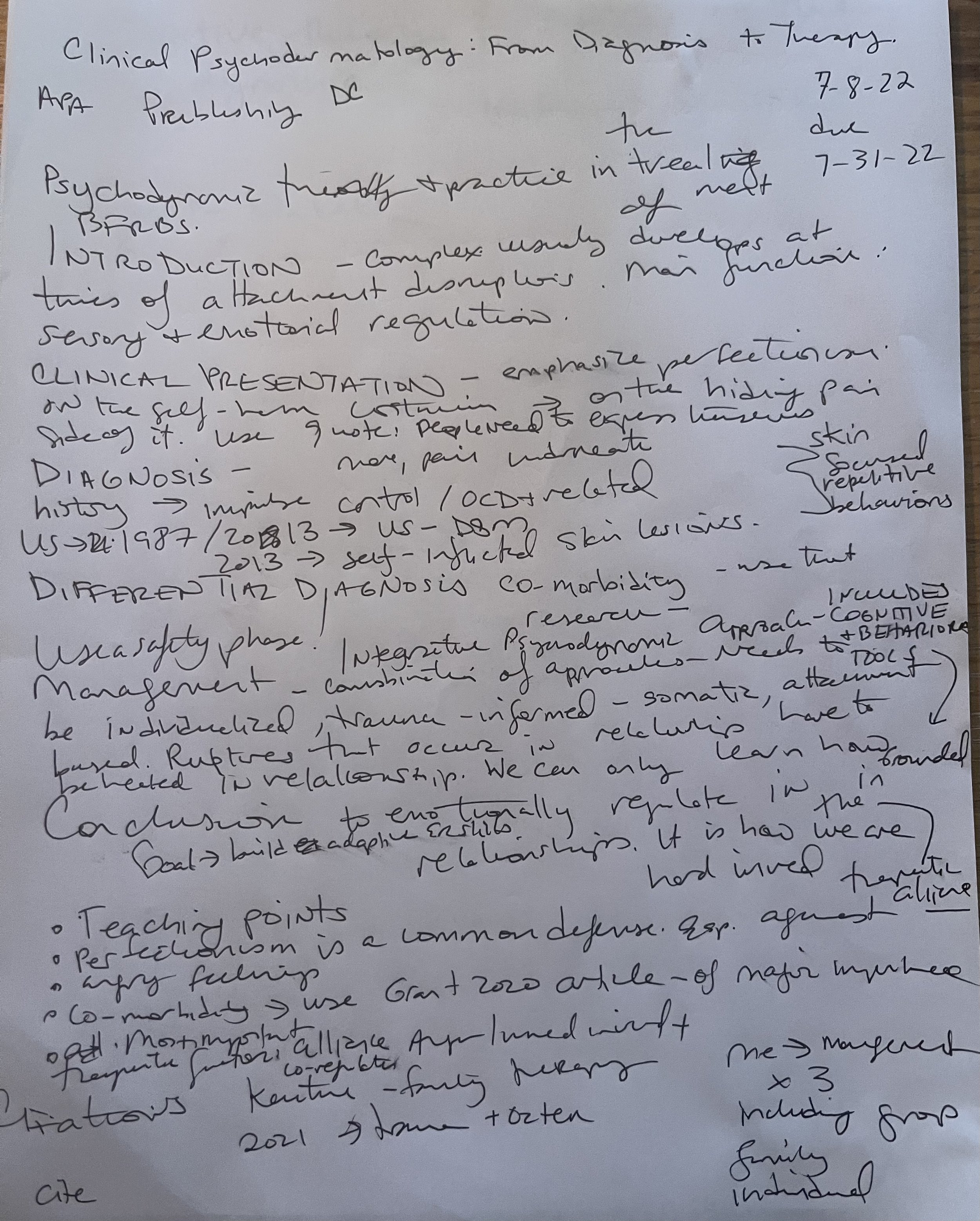
My chapter will cover 6 categories: introduction to BFRBs, clinical presentation, diagnosis, differential diagnosis, management, and teaching points.
I am attaching a draft of the chapter outline. The points I will emphasize:
Perfectionism is a key personality characteristic of those struggling with BFRBs. Perfectionism in this population should be understood as a defense mechanism to hide unwanted feelings, especially anger.
Difficulty with sensory processing is common among those who struggle with BFRBs.
Co-morbidity of other mental health diagnoses, including PTSD, OCD, ADHD, body dysmorphic disorder, anxiety and depression is very high in people struggling with BFRBs. BFRBs serve to regulate emotions, so that they can counteract the various uncomfortable feelings that come up for people with these diagnoses, e.g. help focus the attention for those with ADHD, calm the body down for those struggling with anxiety, or create a trance-like state for those with PTSD to avoid intrusive thoughts.
Precipitating events often include attachment disruptions, including divorce, loss of a beloved grandparent, or traumatic experiences.
Psychodynamic therapy is a good fit for treatment for BFRBs as it addresses attachment disruptions and the therapeutic relationship is key to developing new adaptive emotional regulation skills.
Therapy must go beyond talk therapy to include somatic experience.
I have three weeks to finish the chapter, wish me luck!